Article Text

Abstract
Objective To investigate cognitive inhibition in presymptomatic C9orf72 mutation carriers (C9+) and its associated neuroanatomical correlates.
Methods Thirty-eight presymptomatic C9orf72 mutation carriers (C9+, mean age 38.2±8.0 years) and 22 C9− controls from the PREV-DEMALS cohort were included in this study. They underwent a cognitive inhibition assessment with the Hayling Sentence Completion Test (HSCT; time to completion (part B−part A); error score in part B) as well as a 3D MRI.
Results C9+ individuals younger than 40 years had higher error scores (part B) but equivalent HSCT time to completion (part B−part A) compared to C9− individuals. C9+ individuals older than 40 years had both higher error scores and longer time to completion. HSCT time to completion significantly predicted the proximity to estimated clinical conversion from presymptomatic to symptomatic phase in C9+ individuals (based on the average age at onset of affected relatives in the family). Anatomically, we found that HSCT time to completion was associated with the integrity of the cerebellum.
Conclusion The HSCT represents a good marker of cognitive inhibition impairments in C9+ and of proximity to clinical conversion. This study also highlights the key role of the cerebellum in cognitive inhibition.
- C9orf72 mutation
- cognitive inhibition
- hayling sentence completion test
- voxel-based morphometry
- cerebellum
Statistics from Altmetric.com
- C9orf72 mutation
- cognitive inhibition
- hayling sentence completion test
- voxel-based morphometry
- cerebellum
Introduction
Cognitive inhibition refers to the ability to resist to interference from irrelevant stimuli and is critical to manage everyday tasks. The Hayling Sentence Completion Test (HSCT) has been highlighted as an ecological cognitive inhibition task due to its ability to predict everyday functioning1 and its resemblance to real-life inhibitory demands, such as the ability to suppress inappropriate words, which is part of many social interactions.2 Clinically, the HSCT has been used in many populations presenting with disinhibition, such as patients with Alzheimer’s disease, Parkinson’s disease, progressive supranuclear palsy, bipolar disorder and finally, patients with cerebrovascular accidents or tumours.3–7 Neuroimaging studies suggest that the HSCT is mainly associated with frontal damage.5–11 In patients with frontotemporal dementia (FTD), the HSCT has also shown to be highly sensitive to cognitive inhibition impairments.8–12
The HSCT therefore represents an interest for presymptomatic carriers of chromosome 9 open reading frame 72 (C9orf72) mutation, which is the most frequent genetic cause of FTD and amyotrophic lateral sclerosis (ALS).13 14 Little is known on cognitive inhibition abilities of presymptomatic individuals carrying C9orf72 expansion (C9+), and very few studies have investigated cognition in general at this very early stage of FTD and ALS. While some authors did not detect any cognitive change in these pre-symptomatic individuals,15–17 others have identified specific cognitive changes in executive, praxis or memory even many years before the expected disease onset (for a review, see table 1).18–21 All together, these studies have provided inconsistent results across cognitive functions, and no study has identified a direct relationship between cognitive and neuroanatomical changes.
Review of studies investigating cognitive changes in presymptomatic C9+ vs C9− individuals
Many neuroimaging studies have demonstrated that even if still in the presymptomatic phase, C9+ individuals already present with brain damage in frontal, temporal and parietal lobes as well as the thalami, the caudate nuclei, the cerebellum, the striatum and several white matter fascicles.15–23 In particular, subtle cognitive, structural and microstructural alterations can be detected very early in C9orf72 carriers younger than 40 years.18 However, despite the growing interest in these populations of individuals likely to be treated before developing the disease, there are still no relevant clinical and cognitive tools to detect early signs of impairments or able to predict the proximity to clinical conversion.
Within this framework, our aims were (1) to study cognitive inhibition performances in a large group of C9+ individuals using the HSCT, (2) to explore HSCT performances splitting C9 individuals according to age (younger and older than 40 years, the latter group supposed to be closer to the disease onset), (3) to determine the ability of the HSCT to predict proximity to estimated clinical conversion from presymptomatic to symptomatic phase in C9+ individuals (based on the average age at onset of affected relatives in the family) and (4) to investigate the neuroanatomical correlates of cognitive inhibition as assessed by the HSCT.
We hypothesised that all C9+ individuals would be impaired on the HSCT compared to C9− healthy subjects (including individuals under the age of 40 years), that the HSCT could be a useful tool to predict estimated time to disease onset in C9+ individuals and that frontal regions would be correlated with poor cognitive inhibition.
Methods
Participants
Subjects from the PREV-DEMALS national multicentric study with available HSCT and MRI data were included in the present study. Only the subjects investigated in one centre, Pitié-Salpêtrière hospital, were included. All the details of the study have been previously described.18
Sixty first-degree relatives of C9orf72 mutation carriers from 37 families were included. Thirty-eight participants carried a pathogenic expansion (>23 GGGGCC repeats; C9+); 22 healthy controls did not carry this expansion (C9−). Expected ages at onset of C9+ were estimated by subtracting the age of the participant at assessment to the mean age at symptoms onset within the family, as performed in other studies.21 Demographic and general cognitive characteristics are presented in table 2.
Demographic characteristics
Cognitive study
Hayling Sentence Completion Test
Cognitive inhibition was assessed using the francophone version of the HSCT, a test consisting of two parts in which participants are asked to complete a series of sentences.24 25 In part A (initiation condition), participants must complete 15 sentences as quickly as possible using the contextually predicted word (eg, “The postman was bitten by a”; Response: Dog). In part B (inhibition condition), participants must complete 15 sentences as rapidly as possible using a completely unconnected word, which requires inhibiting an automatic response. Two outcome measures were calculated: (1) the total time in seconds taken to complete every sentence in part A subtracted from the total time taken to complete every sentence in part B (time to completion (part B−part A)); (2) an error score for the part B computed using the scoring system suggested by Burgess and Shallice.24 A 3-point error score was given for an item in which the participant completed the sentence using the predicted word. A 1-point error score was given for an item in which the participant completed the sentence using a semantically related word. A 0-point error score was given for good responses. Thus, for both outcome measures, a higher score indicates a worse performance.
Statistical analyses
The first analysis aimed at comparing the performance of presymptomatic C9+ and C9− individuals on the HSCT, taking into account the dependence of observations from individuals in the same family (cluster effect) and controlling for age, sex and education. Group means were estimated using generalised estimated equations (GEEs) with an exchangeable covariance structure and a multivariable linear regression analysis (distribution: normal; link function: identity). Performance on the HSCT was the dependent variable and group (C9+/C9−), age, sex and education were the predictors. The estimated group means were compared with a statistical threshold of p value ≤0.05. Two separate GEE models were computed: one using time to completion (part B−part A) as a measure of HSCT performance and one using the error scores (part B). This analysis was first conducted on the whole group, then separating individuals based on age (younger and older than 40 years) to determine the effect of age. We chose a cut-off of 40 years old based on the average of age in our population and also to remain consistent with a previous study from our group.18
The second analysis aimed at assessing the ability of the HSCT performance to predict proximity to estimated clinical conversion from presymptomatic to symptomatic phase in C9+ individuals (based on the average age at onset of affected relatives in the family), taking into account the dependence of observations from individuals in the same family (cluster effect) and controlling for sex and education. We performed GEEs using an exchangeable correlation structure, a normal distribution and an identity link function. Expected time to disease onset was the dependent variable and HSCT performance, sex and education were the predictors. Two separate GEE models were computed: one using time to completion (part B−part A) as a measure of HSCT performance and one using the error scores.
MRI study
Acquisition
All scans were acquired on a Siemens Prisma Syngo 3T. Parameters of the 3D T1 sequence were as follows: spatial resolution=(1.1×1.1×1.1) mm3; TE/TR=2.8–3 ms/minimum; bandwidth: 240–255 Hz.
Voxel-based morphometry: pre-processing
Structural images were preprocessed using voxel-based morphometry (VBM) implemented in SPM12 using MATLAB V.7.14.0.739 (Mathworks, Natick, MA). The images were segmented into grey (GM) and white matter. Affine registered tissue segments were used to create a custom template using the DARTEL (diffeomorphic anatomical registration using exponentiated lie algebra) approach.26 For each participant, the flow fields were calculated during a template creation, which described the transformation from each native GM image to the template. These were then applied to each participant’s GM image. The VBM analysis was based on modulated GM images, where the GM value for each voxel was multiplied by the Jacobian determinant derived from spatial normalisation to preserve the total amount of GM from the original images.27 The resulting modulated and normalised images were then smoothed with a Gaussian kernel of 8 mm full width at half maximum.
Statistical analyses
Whole-brain VBM analyses were performed on smoothed GM images. First, the HSCT time to completion (part B−part A) and error score were entered as covariates of interest in two separate multiple regression statistical models including all subjects, with age, sex and total intracranial volume as nuisance covariates. The correlation was tested using a [−1] t-contrast, assuming that higher scores (which indicate worse performances) would be associated with decreased GM volumes. The significance of each effect of interest was determined using the theory of Gaussian fields. A statistical threshold of p value ≤0.05 family-wise error rate (FWE) corrected at cluster level was used.
Results
Group comparison of performance on the HSCT
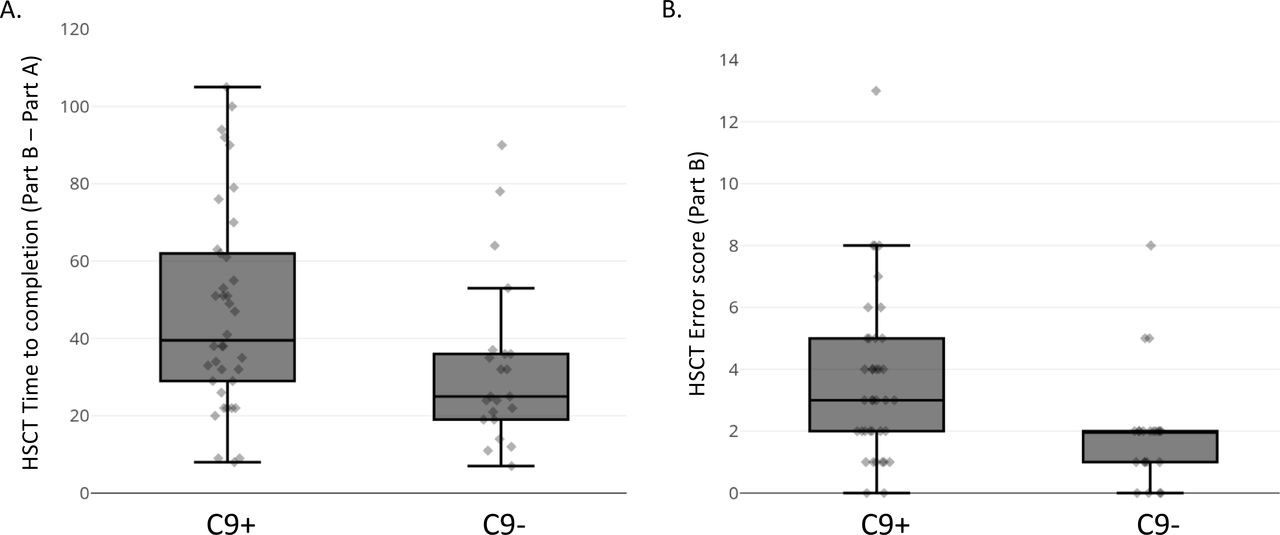
C9+ individuals presented a significantly slower mean HSCT time to completion (part B–part A) in comparison with C9− individuals (p≤0.05) (table 3, figure 1). C9+ individuals also presented significantly higher HSCT error scores (part B) in comparison with C9− individuals (p≤0.001) (table 3, figure 1). Of note, C9− individuals obtained results on the HSCT that were largely comparably with those of the healthy controls previously published (error score: 2.0±1.9 in the present study vs 2.3±4.2).12 To confirm that these results were not biased by outliers, we identified any data points that are more than 1.5 box-lengths (or IQR) from the edge of their group boxplot (figure 1). For HSCT time to completion, there were three outliers in the C9− group. For HSCT error scores, there were one outlier in the C9+ group and three outliers in the C9− group. When these outliers were removed from the analyses, the results were still significant (ie, significantly higher HSCT time to completion and error scores in C9+ individuals).
Group comparisons of performance on the HSCT

Performance on the Hayling Sentence Completion Test (HSCT) in C9− and C9+.
When restricting the same analyses to participants younger than 40 years (C9+ n=22, mean age=32.7±5.2, mean expected time to onset=24.9±7.9; C9− n=12, mean age=31.9±5.9), C9+ individuals presented equivalent time to completion (part B–part A) in comparison with C9− individuals (p=0.297), but they had higher error scores (p=0.034). In participants older than 40 years (C9+ n=16, mean age=45.7±4.2, mean expected time to onset=15.7±5.8; C9− n=10, mean age=50.3±6.8), both HSCT time to completion (p<0.001) and error score (p<0.001) were higher in C9+ in comparison with C9− individuals.
Ability of the HSCT performance to predict expected time to disease onset in C9+ individuals
In C9+ individuals, HSCT completion time (part B–part A) significantly predicted expected time to disease onset (β=0.143 (±0.05); Wald χ2=7.88; df=1; p=0.005). Sex and education were not significant predictors. Overall, this suggests that higher HSCT completion time predicts the proximity to disease onset in C9+ individuals, in agreement with our previous result on C9+ older than the age of 40 years. HSCT error score did not significantly predict expected time to disease onset (β=0.925 (±0.48); Wald χ2=3.78; df=1; p=0.052).
Neuroanatomical correlates of HSCT performance
HSCT time to completion (part B–part A) correlated with GM volume in a large cluster in the left cerebellum (p≤0.05 FWE cluster level corrected; cluster extent: 2132 voxels). Peak significance was observed in the left cerebellar lobule VI (–18, –57, –14; t=4.93). The cluster also included the left cerebellar lobules IV–V (–5, –45, –12; t=3.94), the left vermis (–3, –66, –10; t=3.36) and the left cerebellar lobule crus I (–13, –68, –27; t=3.29).
The HSCT error score (part B) did not correlate with GM volume in any voxel.
Post hoc analysis: cerebellar GM correlates of HSCT time to completion
The whole-brain VBM analysis identified the left cerebellum as a GM correlate of HSCT time to completion (part B–part A). However, traditional VBM analysis is not ideal to investigate the cerebellum because it relies on the ICBM12 template which provides very little contrast for cerebellar structures and normalisation to this template leads to a large spatial spread of individual fissures.28–31 We therefore ran a post hoc analysis using a toolbox specifically designed to resolve these limitations, the Spatially Unbiased Infratentorial Toolbox (SUIT).28–31 The aims of the post hoc analyses were to (1) confirm the result obtained in our traditional VBM analysis (HSCT time to completion correlated with GM volume in the left cerebellum across our sample) and (2) investigate GM correlates of HSCT in C9+ individuals specifically.
Preprocessing
Preprocessing was conducted using SUIT (V.3.4) implemented in SPM12.28–31 First, the infratentorial area was isolated from the images and segmented into GM and white matter to obtain a cerebellar mask (suit_isolate_seg function). A normalisation of the cerebellar mask to the SUIT atlas space was then conducted (suit_normalize_dartel function). During this step, flow fields (which describe the transformation from each native GM image to the template) are also calculated for each participant. These were then applied to each participant’s GM image to reslice them into the SUIT space (suit_reslice_dartel function with modulation).
Results
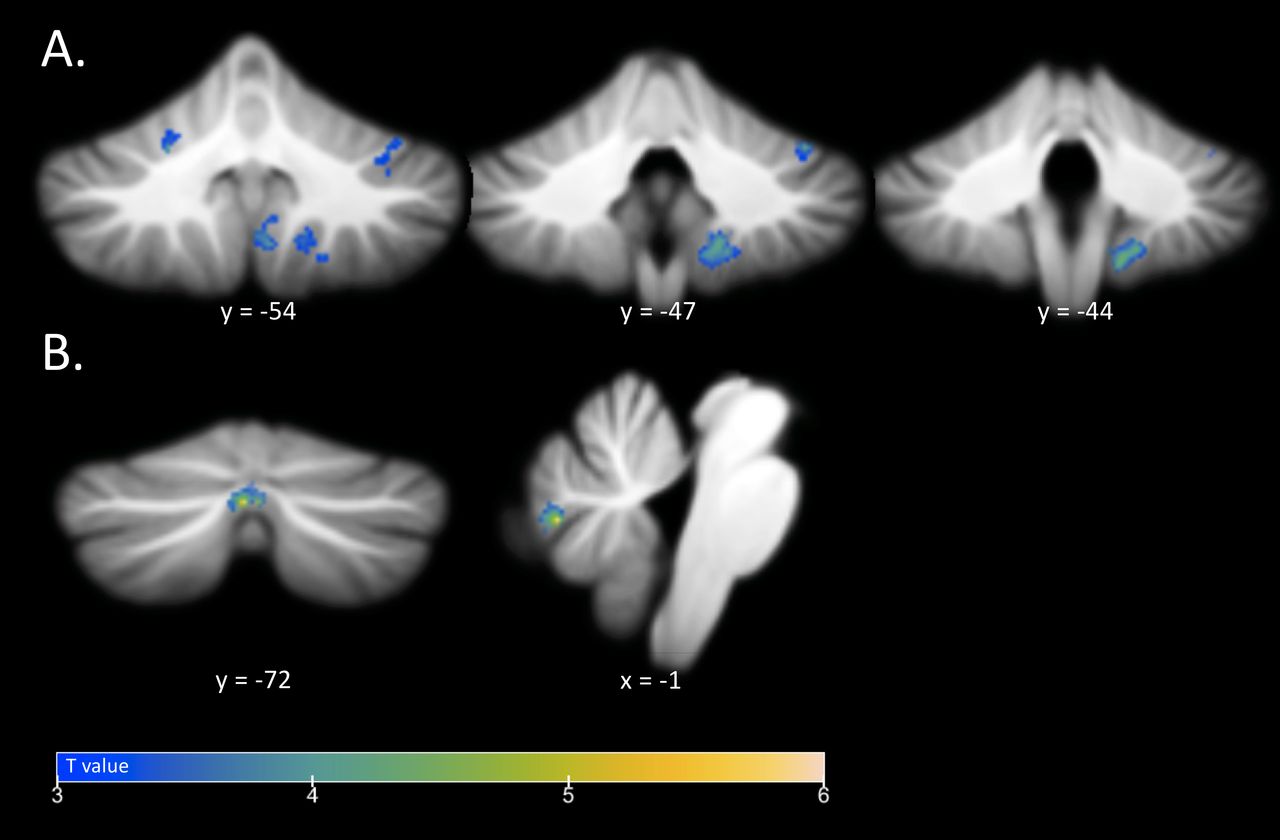
Similarly to the whole-brain VBM analysis, HSCT time to completion (part B–part A) correlated with GM volume in the left cerebellar lobule VI (p≤0.05 FWE cluster level corrected), as displayed in figure 2A and table 4. Three other clusters were also significant, namely the right cerebellar lobule VIIIb, the right cerebellar lobule IX and the right cerebellar lobule VI.

{kind=link}
{kind=link}
Cerebellar regions in which grey matter volume correlates with Hayling Sentence Completion Test time to completion (part B−part A); p≤0.05 FWE cluster level corrected in (A) the complete sample and (B) C9+ individuals.
Cerebellar GM correlates of HSCT time to completion (part B–part A) obtained by using the Spatially Unbiased Infratentorial Toolbox (p≤0.05 FWE cluster level corrected).
When restricting the analysis to C9+ individuals, the correlation between HSCT time to completion and the cerebellum remained significant, although the significant cluster was located in the vermis (p≤0.05 FWE cluster level corrected), as displayed in figure 2B and table 4. Peak significance was observed in the left vermis crus II and the cluster also included the right vermis VIIb.
Discussion
The present study reports on the potential of the HSCT to characterise and detect cognitive inhibition deficits in preclinical settings. We demonstrated that the HSCT was able to discriminate between C9+ and C9− individuals many years before the supposed disease onset (mean expected time to disease onset of 21.1 years), more significantly in individuals over 40 years old who are supposed to be closer to the disease onset. Furthermore, in C9+ individuals, HSCT time to completion significantly predicted estimated time to disease onset. Surprisingly and in contrast with our initial hypothesis, the performance on this test was not associated with frontal areas but with the integrity of the cerebellum, a key region associated with the C9orf72 mutation.
Our study is one of the first to identify a discriminant and early cognitive marker in C9+ individuals (table 1). In previous studies, other neuropsychological tests involving cognitive inhibition functioning such as the Stroop test provided inconsistent results.19 20 The Trail Making Test, which also assesses cognitive flexibility, did not allow for the detection of significant differences between C9+ and C9− individuals.19 20 Other candidates for early cognitive markers in presymptomatic C9+ individuals might include memory and praxis tests (table 1), although their ability to predict estimated proximity to conversion to symptomatic phases and their neural correlates have not been clarified in this population. In presymptomatic MAPT and GRN mutation carriers, letter fluency, categorical fluency and ScreeLing phonology tasks were shown to predict clinical conversion.32 This highlights the interest of the HSCT as an assessment tool in this population and suggests that cognitive inhibition might be among the first cognitive functions showing subtle changes in C9+ individuals. The HSCT was selected because previous studies suggest that it is potentially more ecologically valid than traditional inhibition tests since it has more resemblance to real-life inhibitory demands, as the ability to suppress inappropriate word forms is part of many social interactions.2 Nonetheless, whether the identified cognitive inhibition changes manifest as subtle real-life disinhibition behaviors in C9+ individuals remains to be assessed. Our results are in line with the symptomatic phases of the C9orf72 in which cognitive inhibition impairments play a key role and in which the HSCT is also one of the most discriminative tools.8 10 Furthermore, we have shown that lower performance on the HSCT (slower HSCT time to completion) significantly predicts closer proximity to disease onset in C9+ individuals. The time of completion was also significantly impaired in C9+ individuals older than 40 years, who are supposed to be closer to the disease onset. These findings provide evidence for the HSCT as an easy marker of progression from presymptomatic to symptomatic phase. This test can be easily applied in future studies of potential disease-modifying treatments against FTD and ALS to select the population.
In addition to the utility of the HSCT in the clinical/cognitive assessment of C9+, we showed for the first time that performance on the HSCT is associated with grey matter volume in the cerebellum (ie, lower cerebellar volumes are associated with lower performance). This result is of great significance because recently the cerebellum has been unveiled as playing a key role in the C9orf72 mutation. First, from a pathology perspective, the cerebellum is a key locus of tissue pathology in C9+ patients as demonstrated in many postmortem studies33 34. Moreover, many in vivo studies reported a significant cerebellar atrophy on both presymptomatic20–22 and symptomatic C9orf72 patients.35–39 Functionally, the cerebellum also appears disconnected from different brain networks affected in C9+ individuals, such as the salience, default mode, sensorimotor and medial pulvinar thalamus-seeded networks.19 Connectivity studies have shown that the cerebellum is extensively connected with the prefrontal cortex via the thalamus,40 which are both key regions in FTD. The thalamus, in particular, seems early involved in the pathological brain damage in C9orf72.19 The neural connectivity between these brain regions might explain the correlation between the cerebellum integrity and cognitive inhibition.
Previous studies investigating the neural correlates of cognitive inhibition using the HSCT have mostly highlighted the contribution of prefrontal regions.5–11 Even though the cerebellum has traditionally been considered to be mainly involved in motor abilities, many studies have highlighted its role in cognitive inhibition. In the present study, we found significant associations between the HSCT time to completion (part B–part A) and GM in posterior cerebellar regions (such as the vermis VIIb, vermis crus II, and lobules IX, VI and VIIIb). In this vein, Kansal and colleagues have proposed a detailed mapping of the cerebellum in a large cohort of patients with mixed subtypes of cerebellar neurodegenerative disease,41 and they showed associations between the posterior lobe of the cerebellum and cognitive tasks (vs associations between the anterior lobe of the cerebellum and motor tasks).41 In turn, Reetz and colleagues have shown that the posterior lobe of the cerebellum shows stronger functional connectivity with fronto-temporo-parietal areas, the insula and the thalamus (regions implicated in cognitive and affective processes).42 These previous studies are in line with our results. More generally, brain–behavior relationships between these specific posterior cerebellar regions and cognitive inhibition or executive tasks implying cognitive inhibition have also been reported: Stroop test and GM volume in the vermis crus II,43 go/no-go task and GM volume in the vermis lobule VI44 and finally, Wisconsin Card Sorting task and GM volume in the vermis VIIb.43 Finally, a recent study has also shown that transcranial direct current stimulation over the medial cerebellum reduced the percentage of errors during a go/no-go task.45
Interestingly, cerebellar atrophy has also been associated with other symptoms in C9+ individuals, more precisely with anxiety,46 psychosis47 and deranged body schema processing.48 In this vein, a study recently conducted on patients affected by Friedreich ataxia, a neurodegenerative pathology targeting the dentate nucleus of cerebellum (especially the myelinated efferent white matter fibres), has shown that only the performances on the HSCT were impaired, but not those on other tests assessing the cognitive inhibition (as the Stroop and the Trial Making Test).49 Conversely, a recent study in symptomatic C9+ individuals affected by ALS and also showing cerebellar atrophy did not show any correlation with cognitive symptoms, including cognitive inhibition.50 This result is most probably due to the different neuropsychological measure specifically used in this study (namely the Stroop) and the patients’ clinical phenotype (ALS).
To conclude, the HSCT is a useful tool to detect early cognitive changes in C9+ and to predict the progression from the presymptomatic to the symptomatic phase. Moreover, the observed relationship between impaired performance and cerebellar damage could reflect a disturbance of cortico-thalamo-cerebellar connectivity. More precisely, C9+ individuals might have impaired access to frontal areas critical for successful cognitive inhibition. Future studies should investigate cognitive inhibition using the HSCT on the full spectrum, ranging from presymptomatic subjects to symptomatic patients and possibly using a control group including individuals that do not come from families affected with dementia. Furthermore, future longitudinal studies should directly investigate the potential of the HSCT as a marker of disease progression for the development of new disease-modifying treatments against FTD and ALS. Also, the association between cognitive inhibition impairments and the connectivity between the cerebellum and other key regions in FTD-ALS associated to C9orf72 expansion should be explored.
Acknowledgments
Members of the PREV-DEMALS study group: Carole Aubier Girard (CHU Rouen), Eve Benchetrit (Hôpital Pitié-Salpêtrière, Paris), Hugo Bertin (Hôpital de la Salpêtrière, Paris), Anne Bertrand (Hôpital Pitié-Salpêtrière, Paris), Sandrine Bioux (CHU Rouen), Anne Bissery (Hôpital Pitié-Salpêtrière, Paris), Évangéline Bliaux (CHU Rouen), Stéphanie Bombois (CHU Roger Salengro, Lille), Marie-Paule Boncoeur (CHU Limoges), Pascaline Cassagnaud (CHU Roger Salengro, Lille), Mathieu Chastan (CHU Charles Nicolle, Rouen), Yaohua Chen (CHU Roger Salengro, Lille), Marie Chupin (CATI, ICM, Paris), Olivier Colliot (ICM, Paris), Philippe Couratier (CHU Limoges), Xavier Delbeuck (CHU Roger Salengro, Lille), Vincent Deramecourt (CHU Roger Salengro, Lille), Christine Delmaire (CHU Roger Salengro, Lille), Emmanuel Gerardin (CHU Charles Nicolle, Rouen), Claude Hossein-Foucher (CHU Roger Salengro, Lille), Bruno Dubois (Hôpital Pitié- Salpêtrière, Paris), Marie-Odile Habert (Hôpital Pitié-Salpêtrière, Paris), Didier Hannequin (CHU Charles Nicolle, Rouen), Géraldine Lautrette (CHU Limoges), Thibaud Lebouvier (CHU Roger Salengro, Lille), Isabelle Le Ber (Hôpital Pitié-Salpêtrière Salpêtrière, Paris), Stéphane Lehéricy (Hôpital Pitié-Salpêtrière Salpêtrière, Paris), Benjamin Le Toullec (ICM, Paris), Richard Levy (Hôpital Pitié-Salpêtrière Salpêtrière, Paris), Olivier Martinaud (CHU Charles Nicolle, Rouen), Kelly Martineau (CATI, ICM, Paris), Marie-Anne Mackowiak (CHU Roger Salengro, Lille), Jacques Monteil (CHU Limoges), Florence Pasquier (CHU Roger Salengro, Lille), Grégory Petyt (CHU Roger Salengro, Lille), Pierre-François Pradat (Hôpital Pitié-Salpêtrière, Paris), Dorothée Pouliquen (CHU Rouen), Assi-Hervé Oya (Hôpital Pitié-Salpêtrière, Paris), Daisy Rinaldi (Hôpital Pitié-Salpêtrière, Paris), Adeline Rollin-Sillaire (CHU Roger Salengro, Lille), François Salachas (Hôpital Pitié-Salpêtrière, Paris), Sabrina Sayah (Hôpital Pitié-Salpêtrière, Paris), David Wallon (CHU Rouen).
References
Footnotes
ILB and RM contributed equally.
Contributors Study supervision: ILB, RM. Study conception and design: MM, RM, ILB. Data acquisition: SS, DS, DR, BLT, ILB, AF, AC, PC, MC, DH, CA-G, FP, XD. Analysis and interpretation of data: MM, RM, ILB, SS, BB, OC, AB. Drafting the manuscript: MM, RM, ILB. Obtaining funding: ILB, OC, AB. All authors critically revised the manuscript for its intellectual content.
Funding This study was funded by grant ANR/DGOS PRTS 2015-2019 PREV-DEMALS from the Assistance Publique–Hôpitaux de Paris (Dr Le Ber) and by grant ANR-10-IAIHU-06 from the Agence Nationale de la Recherche. The study was conducted with the support of the Centre d’Investigation Clinique and the Centre pour l’Acquisition et le Traitement des Images platform. Raffaella Migliaccio is supported by France Alzheimer and Philippe Chatrier Foundations, and by Rosita Gomez association. Raffaella Migliaccio, Richard Levy and Bénédicte Batrancourt are supported by Fondation pour la Recherche Medicale. Maxime Montembeault is supported by postdoctoral fellowships from the Canadian Institutes of Health Research (CIHR) and Fonds de Recherche du Québec en Santé (FRQS).
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval This study was approved by the Comité de Protection des Personnes Ile de France VI of the Hôpital Pitié-Salpetrière.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request (isabelle.leber@upmc.fr).